Associate Nurse Manager Parkland Hospital Dallas, Texas, United States
Disclosure(s):
Lauren Huset, BSN, RN, ONC, CNOR: No financial relationships to disclose
Description: Clinical Significance: Local Anesthetic Systemic Toxicity (LAST) is a potentially life-threatening adverse reaction that can result from several factors including exceeding the maximum dosage of local anesthetic. Multiple care teams are involved in the care of patients in the perioperative area including the operating room nurses, scrub techs, anesthesia providers, block team, and surgeons. All these team members come together to prevent LAST in patients undergoing total hip and total knee replacements.
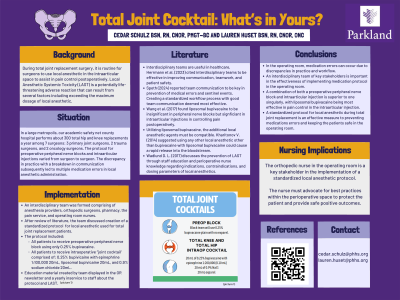
Background: In a metropolitan area, an academic safety net county hospital performs about 300 total hip and knee replacements a year. Our orthopedic program has three primary joint replacement surgeons, with two trauma surgeons and two orthopedic oncology surgeons completing replacements for our patients. Previously, the practice of providing intraoperative local anesthetics and preoperative nerve blocks varied among the providers. The difference in practices led to frequent need for communication between the anesthesia team, block team, surgical team, and surgeon. Medication choices and the amounts given varied between providers and anesthesia staff. Subsequently, due to a breakdown in communication combined with unacquainted teams to the total joint service and local anesthetic protocols, a patient received local anesthetic exceeding the maximum dose for their body weight. The error led to the patient needing additional monitoring post operatively. Question: "Will a standardized protocol for local anesthetic in total joint replacement created by an interdisciplinary team help prevent medication errors in arthroplasty patients?" Description of EBP Protocol: Following the error, an interdisciplinary team was created to review current practices and protocols, conduct a literature review, and implement evidence-based practices in our facility to prevent LAST in our total hip and total knee arthroplasty patients. The interdisciplinary team included the anesthesia faculty over the block team, total joint primary nurses, pain management RN, circulator RNs, operating room manager, and total joint surgeons. During the review of current literature it was found that standardizing the local anesthetic given by all surgeons at a facility helps to reduce deviation from the set protocol and will minimize patient risk. To implement a standardized protocol, the team decided to use only 0.25% plain bupivacaine in all nerve blocks for patients undergoing total hip and total knee arthroplasty in the pre-operative area. The OR team would then give the standardized local injection cocktail to the field for all total hip and knee surgeries for all surgeons. The injection medication cocktail implemented was 20mL of 0.25% bupivacaine with epi1:200,000, 20mL of liposomal bupivacaine, and 20mL of injectable saline. In the pyxis, kits were created with these medications to be dispensed for the nurses to easily gather the correct injection medications. Additionally, a lecture and PowerPoint was provided to the OR surgical team about the standardized protocol. Conclusion/
Discussion: Since the implementation of a standardized protocol for local anesthetic given to total hip and knee arthroplasty patients at an academic county hospital, we have had zero reported errors. As we continue to have new staff, students, surgical residents, and anesthesia residents in the perioperative space, we plan to reinforce the standardized protocol with staff huddles, newsletters, and signs.