Clinical Nurse III New York Presbyterian Morgan Stanley Children's Hospital New York, New York, United States
Disclosure(s):
Valerie Talangbayan, MLA, BSN, RN, CNOR-Ped: No financial relationships to disclose
Description:
Background: Congenital hearing loss is the most common birth defect occurring in 1-3 infants per 1000 births. There are limited options for the treatment of congenital hearing loss. The last major development for the treatment of children with congenital deafness was made in 1990 when cochlear implantation was federally approved in the United States for children, six years after it was approved for adults. Globally, cochlear implantation has been life changing for hundreds of thousands of people. As revolutionary as it has been, cochlear implantation, the hearing it provides is different insofar as it is not like "natural" hearing. The next major breakthrough and development for the treatment of congenital deafness has officially arrived. After years of trials to restore hearing in animals using gene therapy, clinical studies and trials in humans have begun; history is being made. The first group of children to be treated with gene therapy for hearing loss have a specific type of hearing loss. The OTOF gene encodes otoferlin, the protein found in the hair cells of the cochlea essential for neuro transmission. The mutation on the otoferlin gene is know as DVNB9 deafness. It is an autosomal recessive deafness. This type of deafness accounts for 2-8% of all cases of genetic deafness.
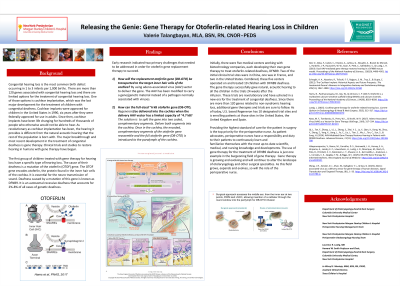
FINDINGS There are certain biomedical challenges that were identified when it comes to this gene therapy. First, how will the gene that needs to be introduced to the hair cells in the cochlea. The solution to the delivery system challenge is the adeno-associated virus (AAV). Second, the size of the otoferlin gene is quite large and poses a different issue. How can the large gene be delivered into the cochlea when the delivery vehicle (AAV) is much smaller than the gene itself. Different groups of scientists have resolved this problem by splitting the gene into different segments. The different segments of the gene are introduced to the target area. The segments have been coded to find their matching, complementary counterpart. Once in the cochlea, the segments reassemble to create the complete gene.
Conclusion: Internationally, there are five medical centers working with different biotechnology companies, each developing its' own gene therapy for this specific congenital deafness. Two of the clinical trial sites are in China, one is in France and two are in the United States. Combined, the five centers have operated on and treated 19 children with DFNB9 deafness. For the most part, the results have been successful in restoring hearing. Clinicians and researchers interested in gene therapy have been patiently awaiting the results of these trials. These promising results have opened up the brave, new world of gene therapy and possibilities for the treatment of other forms of deafness. As the use of gene therapy expands, grows and becomes more established, so will the essential role of the perioperative nurse.

.jpg "Valerie Talangbayan, MLA, BSN, RN, CNOR-PED (she/her/hers) photo")